Cms 1763 Form Printable
Cms 1763 Form Printable - You may also use the search feature to more quickly locate information for a specific form number or. Form cms 1763, request for termination.part b immunosuppressive drug coverage author: Form cms 1763 request for termination of premium hospital and or suppl. Hard copy forms may be available from intermediaries, carriers, state agencies, local. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. First, you will need to fill out a medicare form cms 1763. The form requires your name, medicare. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. Request for termination of premium hospital insurance of. Many cms program related forms are available in portable document format (pdf). The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. The following provides access and/or information for many cms forms. What do you use medicare form cms 1763 for? The form requires your name, medicare. Find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. This form may be outdated. This form is used to terminate the hospital and or medical insurance benefits you. The completion of this form is needed to document your voluntary request for termination of medicare coverage. Form cms 1763 request for termination of premium hospital and or suppl. The form requires your name, medicare. Hard copy forms may be available from intermediaries, carriers, state agencies, local. Back to cms forms list; This form may be outdated. The following provides access and/or information for many cms forms. The form requires your name, medicare. Many cms program related forms are available in portable document format (pdf). What do you use medicare form cms 1763 for? Cms 1763 dynamic list information. Hard copy forms may be available from intermediaries, carriers, state agencies, local. Find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. Form cms 1763 request for termination of premium hospital and or suppl. Many cms program related forms are available in portable document format (pdf). Back to cms forms list; The completion of this form is needed to document your voluntary request. The form requires your name, medicare. Use fill to complete blank. What do you use medicare form cms 1763 for? Form cms 1763, request for termination.part b immunosuppressive drug coverage author: The completion of this form is needed to document your voluntary request for termination of medicare coverage. Use fill to complete blank. This form is used to terminate the hospital and or medical insurance benefits you. Hard copy forms may be available from intermediaries, carriers, state agencies, local. Back to cms forms list; The following provides access and/or information for many cms forms. Download and print the cms 1763 form to request the termination of your medicare coverage for hospital and/or supplementary medical insurance. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Back to cms forms list; The completion of this form is needed to document. Many cms program related forms are available in portable document format (pdf). The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Hard copy forms may be available from intermediaries, carriers, state agencies, local. What do you use medicare form cms 1763 for? Form cms. The form requires your name, medicare. This form may be outdated. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Form cms 1763, request for termination.part b immunosuppressive drug coverage author: Form cms 1763 request for termination of premium hospital and or suppl. The completion of this form is needed to document your voluntary request for termination of medicare coverage. Many cms program related forms are available in portable document format (pdf). Request for termination of premium hospital insurance of. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of. Form cms 1763, request for termination.part b immunosuppressive drug coverage author: The following provides access and/or information for many cms forms. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Request for termination of premium hospital insurance of. Form cms 1763 request for termination. Form cms 1763 request for termination of premium hospital and or suppl. Request for termination of premium hospital insurance of. This form may be outdated. Use fill to complete blank. The completion of this form is needed to document your voluntary request for termination of medicare coverage. This form is used to terminate the hospital and or medical insurance benefits you. Many cms program related forms are available in portable document format (pdf). You may also use the search feature to more quickly locate information for a specific form number or. Download and print the cms 1763 form to request the termination of your medicare coverage for hospital and/or supplementary medical insurance. Find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Back to cms forms list; First, you will need to fill out a medicare form cms 1763. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Cms 1763 dynamic list information. The following provides access and/or information for many cms forms.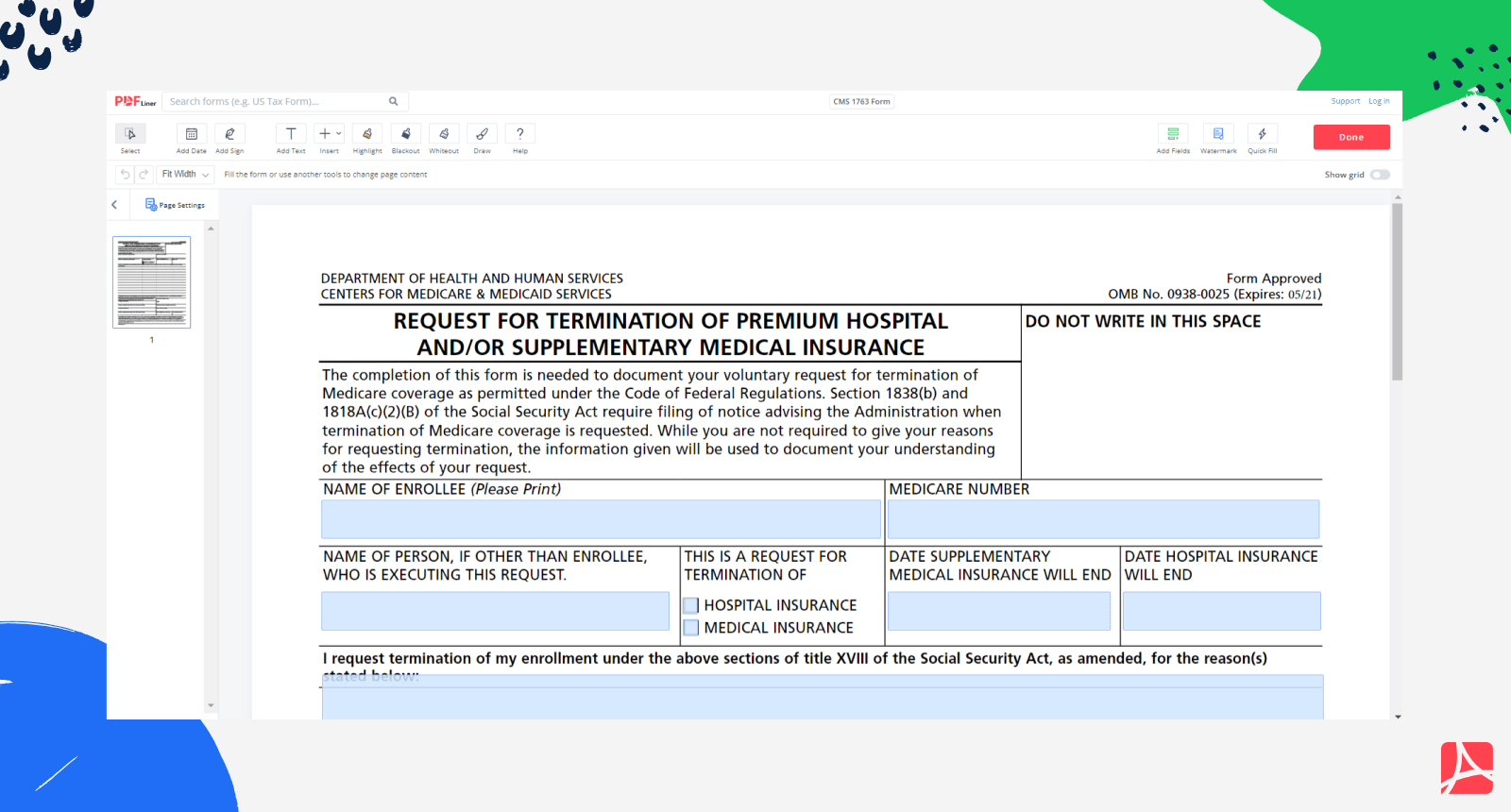
CMS 1763 Form Medicare Form CMS 1763 blank, sign online — PDFliner

Fill Medicare & Medicaid
Form CMS1763 Download Fillable PDF or Fill Online Request for
Form Cms 1763 Fillable Printable Forms Free Online

Fill Free fillable Form CMS1763 REQUEST FOR TERMINATION OF PREMIUM

How To Fill Out Medicare Form Cms 1763 Form example download

Completing Form CMS 1763 for withdraw of Medicare YouTube
CMS 1763 Form Termination of Medical Insurance pdfFiller Blog
Form CMS1763 Fill Out, Sign Online and Download Fillable PDF

Cms 1763 Printable Form
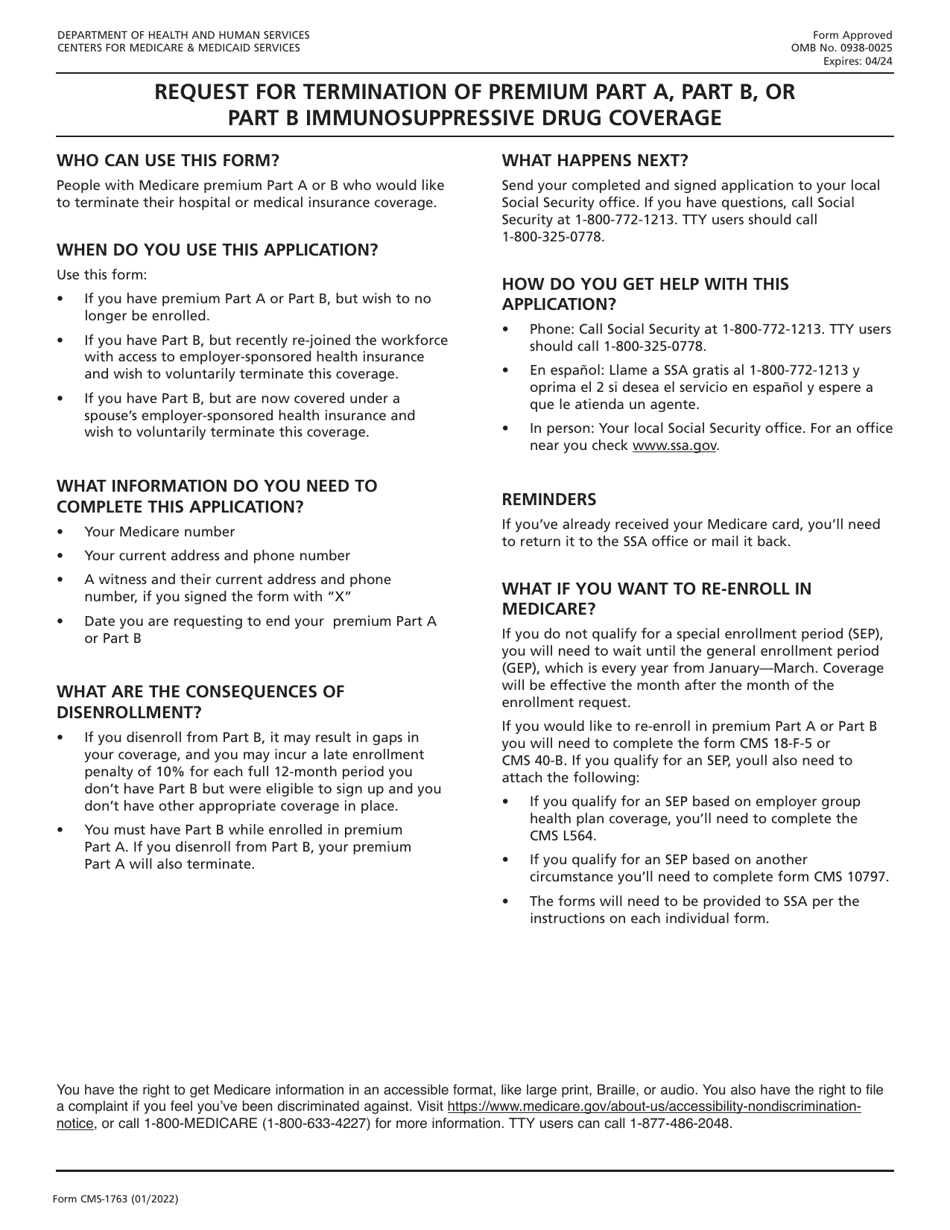
If You Qualify For An Sep, Youll Also Need To Attach The.
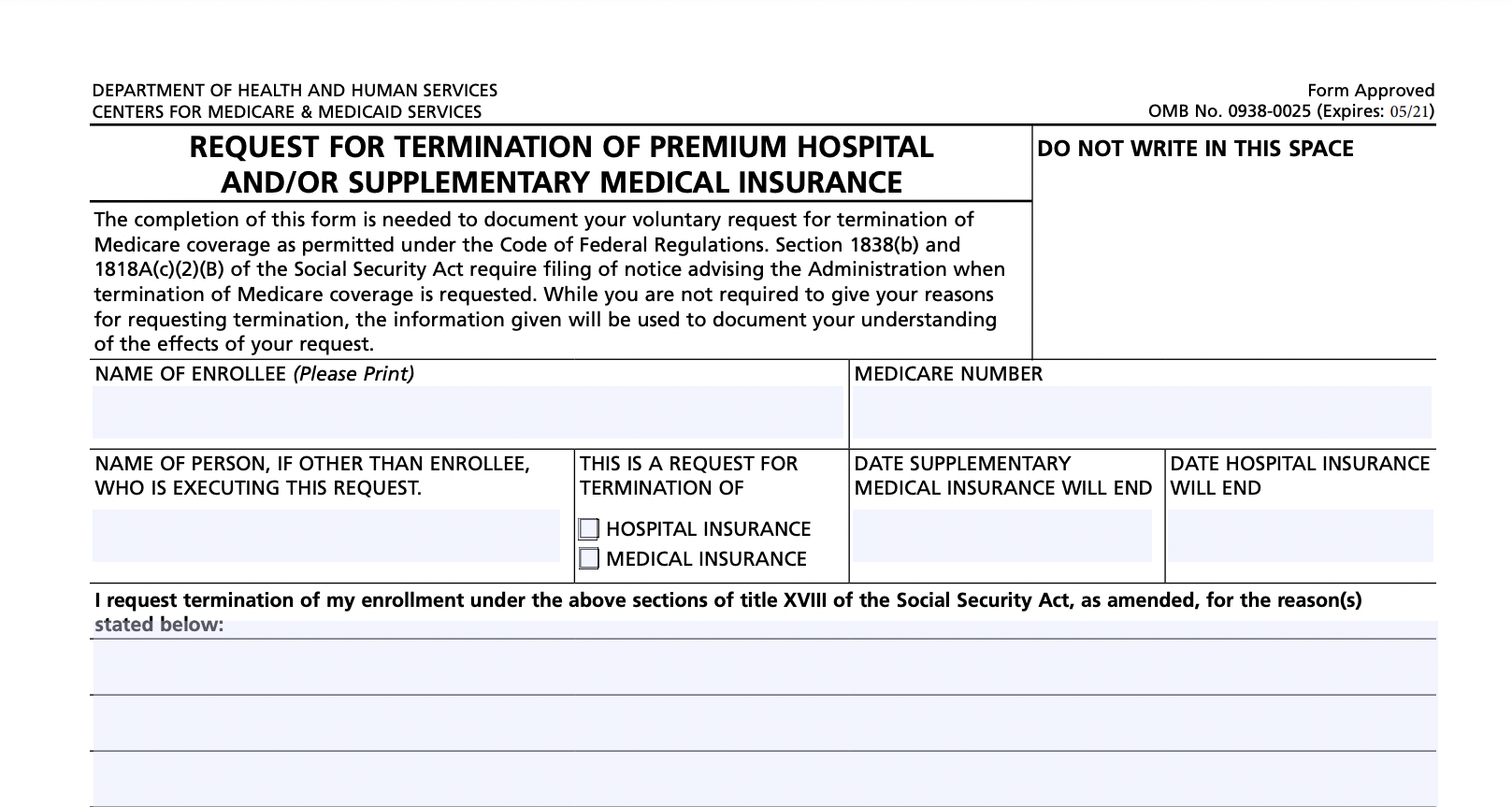
What Do You Use Medicare Form Cms 1763 For?
The Form Requires Your Name, Medicare.
Form Cms 1763, Request For Termination.part B Immunosuppressive Drug Coverage Author:
Related Post: